Future Health Index 2026 - Research Methodology
AI in practice: Shaping the future of healthcare now
Future Health Index 2026 - Research Methodology
AI in practice: Shaping the future of healthcare now
The Future Health Index is commissioned by Philips
In its 11th edition, the Future Health Index 2026 reveals the real-world impact of AI in healthcare and uncovers what is needed to scale these gains. Two quantitative surveys were conducted among over 2,000 healthcare professionals and over 20,000 patients in 10 countries (Brazil, China, France, Germany, India, Indonesia, the Netherlands, Saudi Arabia, the United Kingdom and the United States). The surveys were conducted from February to April 2026.
Research methodology
Research overview and objectives
Over the past decade, the Future Health Index has examined the role of technology in some of the biggest trends health systems have faced. Initially a benchmark of connected care adoption around the world, the Future Health Index has evolved to look at how technology can shape the future of health, based on the perspectives of healthcare leaders, professionals and patients in countries with varying demographics and health systems. In its 11th edition, the Future Health Index 2026 investigates the tangible impact of artificial intelligence on healthcare and the measurable results it delivers. This year’s report moves beyond the potential of AI to highlight how healthcare professionals and patients around the world are actively using AI to regain time, expand capacity, and improve care delivery. The 2026 Future Health Index is based on proprietary quantitative research involving over 2,000 healthcare professionals and over 20,000 patients across 10 countries (Brazil, China, France, Germany, India, Indonesia, the Netherlands, Saudi Arabia, the United Kingdom and the United States). The surveys were conducted from February to April 2026.
The Future Health Index examines a different theme each year, with previous reports focusing on the following areas:
2026 Report: AI in practice: Shaping the future of healthcare now
Two quantitative surveys* were conducted out by Vitreous World, employing a methodology of online (CAWI) surveying. The surveys were conducted from February to April 2026 in 10 countries (Brazil, China**, France, Germany, India, Indonesia, the Netherlands, Saudi Arabia, the United Kingdom and the United States).
2026 quantitative survey methodology
* Two separate surveys were conducted, but for ease, data is referred to as coming from a ‘survey’ in the report. Survey 2: 20,085 patients aged 18+ participated in a 10-minute online survey
**Survey data is representative of Mainland China only and does not include Taiwan or Hong Kong.
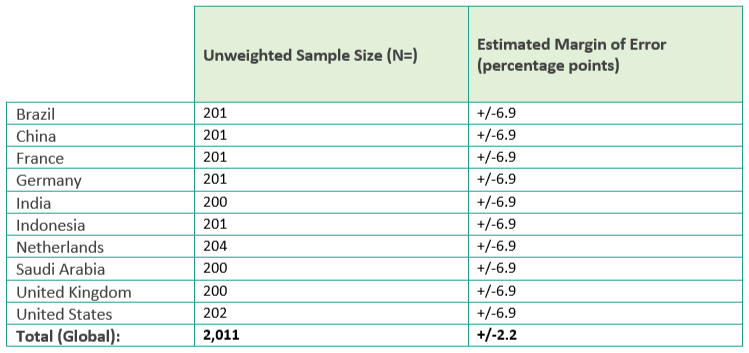
Survey 1: 2,011 healthcare professionals participated in a 15-minute online survey
Where relevant, the surveys were translated into the local language. In some instances, certain questions needed to be adjusted slightly for relevance. Care was taken to ensure the meaning of the question remained as close to the original English version as possible. ***Estimated margin of error is the margin of error that would be associated with a sample of this size for the respondent population in each country.
The below tables show the sample sizes as well as the estimated margin of error*** at the 95% confidence level.
Healthcare professionals survey:
Patient survey:

2025 Report: Building trust in healthcare AI: Perspectives from patients and professionals
Two quantitative surveys were carried out by Accenture Song, the world’s largest tech-powered creative group employing a methodology of online (CAWI) surveying.
2025 quantitative survey methodology
The surveys were conducted from December 2024 to April 2025 in 16 countries (Australia, Brazil, Canada, China*, France, Germany, India, Indonesia, Japan, Netherlands, Saudi Arabia, Spain, South Africa, South Korea, the United Kingdom and the United States).
*Survey data is representative of Mainland China only and does not include Taiwan or Hong Kong.
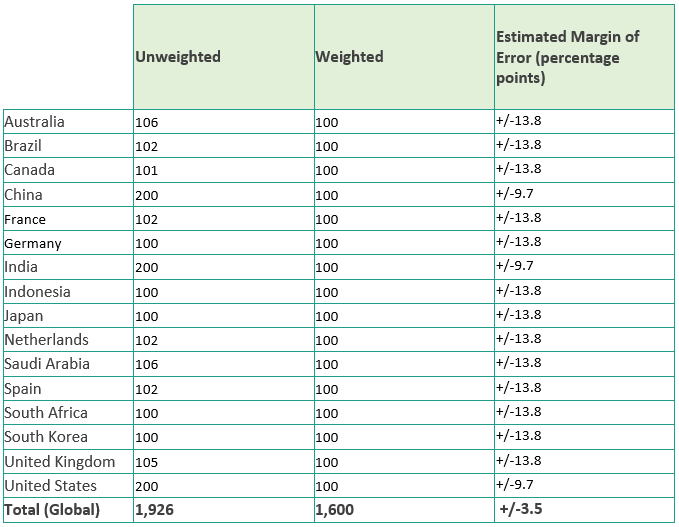
Survey 1: 1,926 healthcare professionals participated in a 15-minute online survey
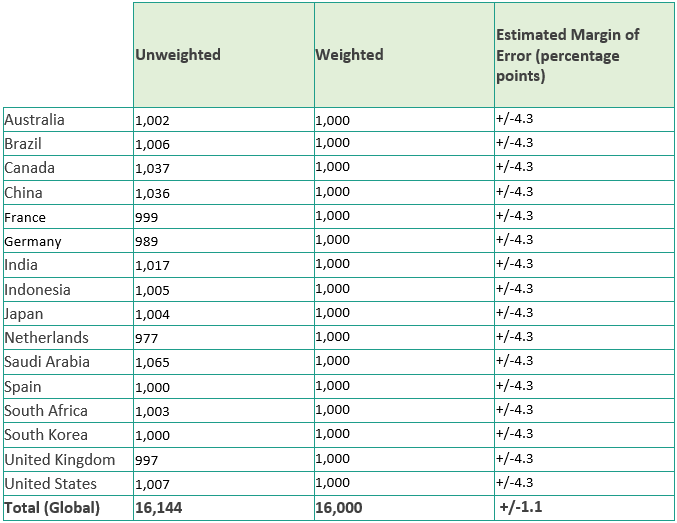
Survey 2: 16,144 patients aged 18+ participated in a 10-minute online survey
Where relevant, the surveys were translated into the local language. In some instances, certain questions needed to be adjusted slightly for relevance within specific countries. Care was taken to ensure the meaning of the question remained as close to the original English version as possible. The below tables show both the unweighted and weighted sample sizes as well as the estimated margin of error** at the 95% confidence level. Please note that this report utilizes weighted data for both healthcare professional and patient surveys to provide insights that are representative across the diverse markets analyzed. **Estimated margin of error is the margin of error that would be associated with a sample of this size for the respondent population in each country.
In both instances – healthcare professionals and patients – sample sizes were weighted to ensure representative results at the global level.
Weighting is a statistical technique used to adjust the sample data to ensure it accurately represents the larger population. This process is vital when certain groups are over- or under-represented in the sample compared to their actual proportions in the population. This:
Healthcare professionals survey:
Patient survey:
2024 Report: Better care for more people: Bridging gaps in healthcare
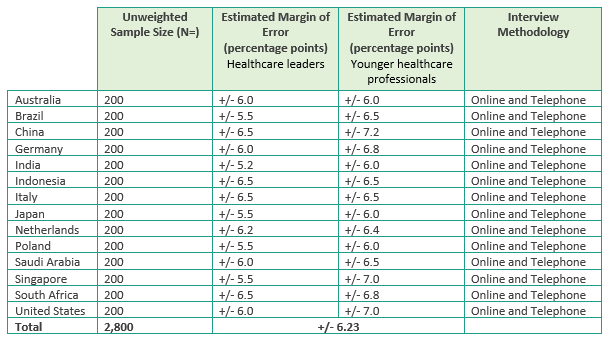
2024 quantitative survey methodology In partnership with GemSeek, a global business and consumer research services organization, a quantitative survey was fielded using an online (CAWI) methodology between December 2023 – February 2024. The survey was answered by 2,800 healthcare leaders, 200 in each of the 14 countries included (Australia, Brazil, China**, India, Indonesia, Italy, Japan, the Netherlands, Poland, Saudi Arabia, Singapore, South Africa, the United Kingdom and the United States). Where relevant, the survey was translated into a local language and in some instances, questions needed to be adjusted slightly for relevance within specific countries. Care was taken to ensure the meaning of the question remained as close to the original, English, version as possible. Below is the specific sample size, estimated margin of error*** at the 95% confidence level, and interviewing methodology used for each country.
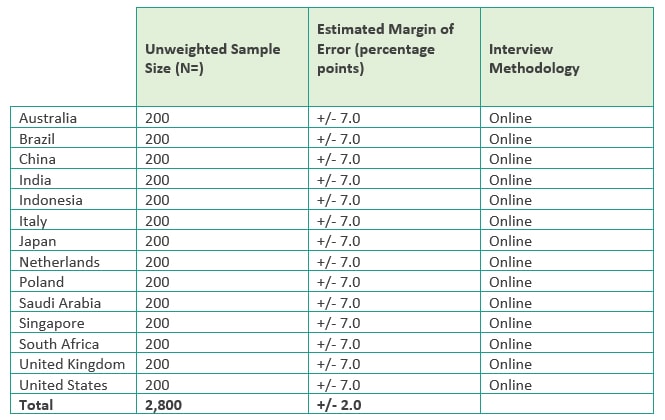
***Estimated margin of error is the margin of error that would be associated with a sample of this size for the full healthcare leader population in each country. However, this is estimated since robust data is not available on the number of healthcare leaders in each country surveyed.
2024 qualitative interview methodology The qualitative portion of the Future Health Index 2024 was also conducted by GemSeek. To provide context and additional depth to the quantitative data, the survey results were supplemented with findings from a series of 45-minute, English-language interviews with healthcare leaders. These sessions were conducted February – March 2024. There were eight participants, two from each of the following countries: Singapore, South Africa, the United Kingdom, and the United States.
2023 Report: Taking healthcare everywhere
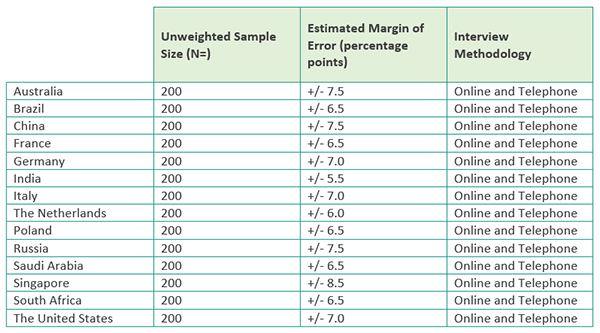
2023 quantitative survey methodology In partnership with iResearch Services, a global business and consumer research services organization, a survey was fielded from December 2022 – February 2023 in 14 countries (Australia, Brazil, China**, Germany, India, Indonesia, Italy, Japan, the Netherlands, Poland, Saudi Arabia, Singapore, South Africa and the United States) in their native language. The survey used a mixed methodology of online and telephone across all countries (as relevant to the needs of each country). 100 healthcare leaders and 100 younger healthcare professionals in each of the 14 countries completed the survey. The total sample from the survey includes: Below is the specific sample size, estimated margin of error* at the 95% confidence level, and interviewing methodology used for each country.
Question localizations In some instances, certain questions needed to be adjusted slightly for relevance within specific countries. Care was taken to ensure the meaning of the question remained as close to the original, English version, as possible.
2022 Report: Healthcare hits reset
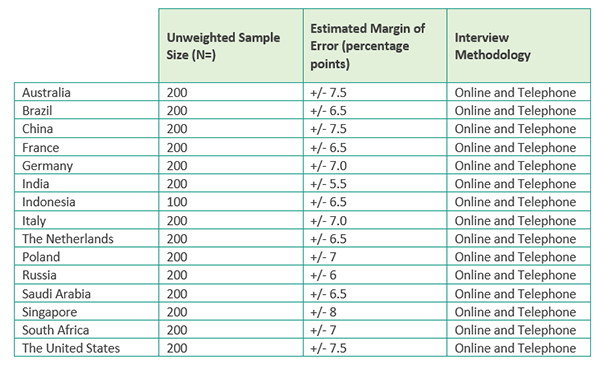
2022 quantitative survey methodology In partnership with iResearch Services, a global business and consumer research services organization, a survey was fielded from December 2021 – February 2022 in 15 countries (Australia, Brazil, China, France, Germany, India, Indonesia, Italy, the Netherlands, Poland, Russia, Saudi Arabia, Singapore, South Africa and the United States) in their native language. The survey used a mixed methodology of online and telephone across all countries (as relevant to the needs of each country). 200 healthcare leaders in each of the 15 countries completed the survey, except in Indonesia where the total sample was 100.
The total sample from the survey includes:
• 2,900 healthcare leaders (defined as a C-suite or senior executive working in a hospital, medical practice, imaging center/office-based lab, or urgent care facility who is a final decision maker or has influence in making decisions).
Below is the specific sample size, estimated margin of error* at the 95% confidence level, and interviewing methodology used for each country.
Question localizations In some instances, certain questions needed to be adjusted slightly for relevance within specific countries. Care was taken to ensure the meaning of the question remained as close to the original, English version, as possible. 2022 qualitative interviews methodology
The qualitative portion of the Future Health Index 2022 was conducted by the KJT Group, a market research and consulting firm which specializes in the healthcare industry. To provide context and additional depth to the quantitative data, the survey results were supplemented with findings from a series of 45-minute interviews with healthcare leaders in their native language. These interviews were conducted during the month of March 2022. There were 30 participants, six from each of the following markets: Australia, China, Germany, the Netherlands and the United States.
* Estimated margin of error is the margin of error that would be associated with a sample of this size for the full healthcare leader population in each country. However, this is estimated since robust data is not available on the number of healthcare leaders in each country surveyed.
2021 Report: Healthcare leaders look beyond crises
2021 quantitative survey methodology In partnership with iResearch Services, a global business and consumer research services organization, a survey was fielded from December 8, 2020 – February 16, 2021 in 14 countries (Australia, Brazil, China, France, Germany, India, Italy, the Netherlands, Poland, Russia, Saudi Arabia, Singapore, South Africa and the United States) in their native language. The survey used a mixed methodology of online and telephone across all of the countries (as relevant to the needs of each country) with a sample size of 200 per country. The survey length was approximately 20 minutes. The total sample from the survey includes: • 2,800 healthcare leaders (defined as a C-suite or senior executive working in a hospital, medical practice, imaging center/office-based lab, or urgent care facility who is a final decision maker or has influence in making decisions). Below is the specific sample size, estimated margin of error at the 95% confidence level, and interviewing methodology used for each country.
Question localizations In some instances, certain questions needed to be adjusted slightly for relevance within specific countries. Care was taken to ensure the meaning of the question remained as close to the original, English version, as possible. 2021 qualitative interviews methodology To provide context and key quotes to the quantitative data, the research was supplemented with 30-minute interviews among healthcare leaders in their native language, which was conducted from February 25, 2021 – March 12, 2021. There were 20 participants, four from each of the following markets: China, Germany, India, the Netherlands and the United States. These interviews were conducted in participation with Heart and Mind Strategies. * Estimated margin of error is the margin of error that would be associated with a sample of this size for the full healthcare leader population in each country. However, this is estimated since robust data is not available on the number of healthcare leaders in each country surveyed.
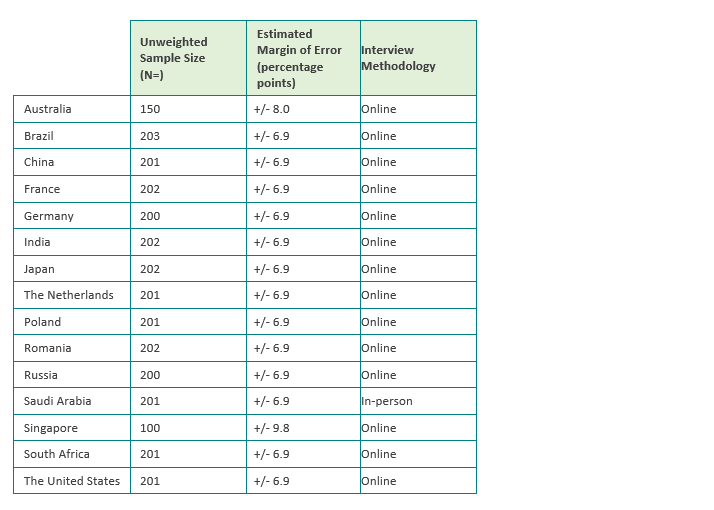
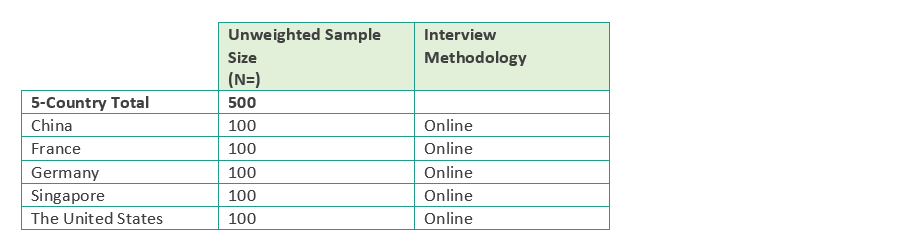
Now in its fifth year, the Future Health Index 2020 report builds on the findings of the previous reports by examining the expectations and experiences of younger healthcare professionals aged under 40 and how they can be empowered to meet the demands of tomorrow’s healthcare. As the first global survey of its kind, the Future Health Index 2020 report features intriguing insights into the next generation of healthcare professionals, a group that will form most of the healthcare workforce over the next 20 years. The research explores this group’s expectations around technology, training and job satisfaction, and the reality of their experience as healthcare professionals. The research for the 2020 Future Health Index was conducted in 15 countries (Australia, Brazil, China[2], France, Germany, India, Japan, the Netherlands, Poland, Romania, Russia, Saudi Arabia, Singapore, South Africa and the United States of America). To provide a holistic understanding of the current healthcare systems around the world, the 2020 study combines quantitative surveys and qualitative online focus groups among the following key stakeholders: · Healthcare professionals in 15 countries (quantitative) · Healthcare professionals in 5 countries (qualitative) The research was conducted prior to the COVID-19 pandemic affecting most of the countries surveyed: To understand the impact of the pandemic on the needs and expectations of this younger group of healthcare professionals, a survey was conducted among doctors aged under 40 years old, who have completed their first medical degree. The survey was fielded from June 19 to July 30, 2020 in 5 countries (China, France, Germany, Singapore and the United States of America) in their native language. The survey was conducted online and offline (as relevant to the needs of each country) with a sample size of 100 per country. The survey length was approximately 10 minutes. The total sample from the survey included 500 doctors under 40 years old. This Insights survey supplements the findings of the Future Health Index 2020 report, launched in March 2020. Taken together, this body of research offers guidance to today’s healthcare leaders on empowering this next generation of professionals to meet the changing demands of modern healthcare. Future Health Index 2020 – Main Study: Quantitative Survey Methodology In partnership with SERMO, an independent global market research firm, a survey was fielded from November 15 to December 27, 2019 in 15 countries (Australia, Brazil, China, France, Germany, India, Japan, the Netherlands, Poland, Romania, Russia, Saudi Arabia, Singapore, South Africa and the United States of America) in their native language. The survey was conducted online and offline (as relevant to the needs of each country) with a sample size of 200 per country for healthcare professionals under 40 years old. The exceptions were Singapore and Australia[1], who each had slightly smaller samples. The survey length was approximately 15 minutes. The total sample from the survey includes: Below is the specific sample size and interviewing methodology used for each country.The 2020 Future Health Index: Main Study & Insights Study
Weighting
The 15-country average is an average calculation whereby each country’s sample size was weighted to have the same value, as such ensuring that each country has an equal weight in this total. The same was done for all regional totals, as well as emerging country and developed country total 1) Country classifications are according to the International Monetary Fund2
Statistical analysis
A statistical analysis was performed to explore the relationship between the type of hospital/practice (in this instance, ‘smart,’ ‘digital’ or ‘analog’) and younger healthcare professionals’ agreement with several questions asked in the Future Health Index 2020 survey. The analysis showed that there is, in fact, a statistical relationship between the type of hospital/practice and certain aspects of their careers. The following survey questions were used for this analysis: To what extent do you agree or disagree with the following? How satisfied or dissatisfied are you in your work as a healthcare professional? A chi-square test of independence was performed for the analysis of each of these survey questions. All results showed the relationship between these variables was significant at the p<.001 level.
Question Localizations
In some instances, certain questions needed to be adjusted slightly for relevance within specific countries. Care was taken to ensure the meaning of the question remained as close to the original, English version, as possible. Future Health Index 2020 – Main Study: Qualitative Interviews Methodology To provide context to the quantitative data (as described above), the research was supplemented with two waves of online focus groups with doctors. Wave one, conducted from January 10, 2020-January 13, 2020, had 36 participants across the following markets: Brazil, the US, France, Germany and Australia. Wave two, conducted from February 3, 2020-February 6, 2020, had 41 participants across the following markets: Brazil, the US, France, Germany and Australia. Online focus groups were conducted in participation with SERMO, an independent global market research firm. Future Health Index 2020 – Insights Study: Quantitative Survey Methodology The survey was conducted from June 19 to July 30, 2020 in 5 countries (China, France, Germany, Singapore and the United States of America) in their native language. The survey was conducted online and offline (as relevant to the needs of each country) with a sample size of 100 per country for doctors under 40 years old, who have completed their first medical degree. The survey length was approximately 10 minutes. The total sample from the survey includes: Below is the specific sample size and interviewing methodology used for each country.
2020 Qualitative Interviews Methodology
To provide context to the quantitative data (as described above), the research was supplemented with two waves of online focus groups with doctors. Wave one, conducted from January 10, 2020-January 13, 2020, had 36 participants across the following markets: Brazil, the US, France, Germany and Australia. Wave two, conducted from February 3, 2020-February 6, 2020, had 41 participants across the following markets: Brazil, the US, France, Germany and Australia. Online focus groups were conducted in participation with SERMO, an independent global market research firm.
2019 Report: Transforming healthcare experiences
Survey data
In partnership with IPSOS and SERMO, independent global market research firms, the surveys were fielded from March 4 to May 19, 2019 in 15 countries (Australia, Brazil, China, France, Germany, India, Italy, The Netherlands, Russia, Saudi Arabia, Singapore, South Africa, Poland, U.K. and U.S.) in their native language. The survey was conducted online and offline (as relevant to the needs of each market) with a sample size of 1,000 per market for the general population and 200 per market for healthcare professionals [1]. The exceptions were the US and Germany, who each had slightly larger samples of healthcare professionals. For the individuals (general population) audience, the survey is representative of key demographics e.g. age, gender, region, location type (i.e. rural/urban), income/SEL/education and ethnicity (where appropriate to ask). This was achieved through a mix of balancing [2] and weighting. In Saudi Arabia and Brazil, the survey is nationally representative of the online population. The survey length was approximately 15 minutes for the US, Germany, and the Netherlands, and approximately 10 minutes for the remaining markets. The total sample from the survey includes: At the 95% confidence level, the 15-country total for the general population has a margin of error at +/- 0.8 percentage points and the 15-country total for the healthcare professional population has an estimated margin of error [3] of +/- 1.7 percentage points. Below is the specific sample size, margin of error at the 95% confidence level, and interviewing methodology used for each market. [2] Interlocking quotas were used for age and gender. All other demographics had non-interlocking quotas. [3] Estimated Margin of Error is the margin of error that would be associated with a sample of this size for the full healthcare professional population in each country. However, this is estimated since robust data is not available on the number of healthcare professionals and specialty mixes in each country surveyed.
[1] For the purposes of this survey, healthcare professionals are defined as those who work in healthcare as a doctor, surgeon, nurse practitioner, registered nurse, licensed practical nurse or nurse across a variety of specializations.
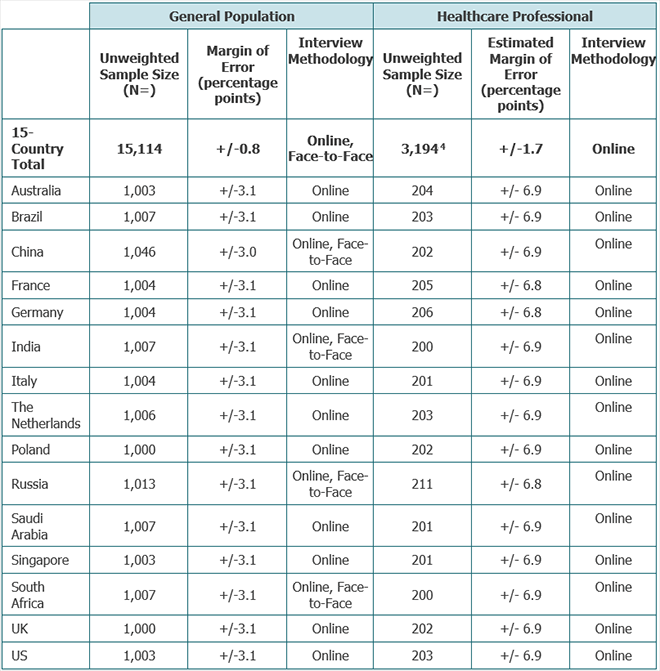
[4] US healthcare professionals sample: 278 in total; this includes an additional sample of 75 healthcare professionals from large hospitals. Germany: healthcare professionals sample: 281 in total; this includes an additional sample of 75 caregivers and nurses. When comparing Germany or the US to other countries the additional samples are removed to ensure samples are comparable. The additional samples are also removed from the 15-country average and any other regional averages.
The Weighting (General Population only)
For the general population sample, all countries were weighted to be representative of the national population based on census statistics (where available) for key demographics. The weighting was applied to ensure the sample is representative of individuals age 18+ in each country. In Brazil and Saudi Arabia, the sample is representative of the online population in these countries.
The 15-country average is an average calculation with each country’s sample size weighted to have the same value to ensure each country has an equal weight in this total. The same was done for all regional totals.
2018 Report 3: Telehealth: Delivering value across institutional and geographical borders
Survey data
For the third report of the Future Health Index in 2018, a variety of third-party sources as well as original research from the 2016 and 2017 Future Health Index data was used. Additionally, data from chapter one of FHI 2018 was also referenced. Please see below for a full list of third-party sources and further details on the survey methodology.
Furthermore, nine key opinion leaders (KOLs) across the Netherlands, US, Spain, France, South Africa, UK and Germany were interviewed to examine the major barriers to telehealth and provide recommendations as to how elements of healthcare can be improved and drive change.
KOLs were chosen on the basis of their industry expertise in relevant areas, such as telehealth and the general healthcare landscape, and were conducted from March 2018 to September 2018 via telephone or video-chat service (e.g. Skype, etc.).
A list of KOLs interviewed is included below:
Franck Baudino, CEO and founder of French telehealth company H4D
Rafael Bengoa, co-director of the Institute for Health & Strategy in Bilbao, Spain, and a senior leadership fellow at Harvard University
2018 Report 2: Moving data to the heart of health systems - Future Health Index report 2018
Survey data
For the second report of the Future Health Index in 2018, a variety of third-party sources as well as original research from the 2016 and 2017 Future Health Index data was used (see survey details below). Additionally, data from chapter one of FHI 2018 was also referenced. A full list of third-party sources, is included below.
Furthermore, 12 key opinion leaders (KOLs) across the Netherlands, US, UK, Australia, Germany, China, Sweden and Estonia were interviewed to provide recommendations and produce tangible guidelines as to how elements of healthcare can be improved and drive change.
KOLs were chosen on the basis of their industry expertise in relevant areas, including connected care technology and the general healthcare landscape, and were conducted from July 20, 2018 to August 9, 2018 via telephone or video-chat service (e.g. Skype, etc.).
A list of KOLs interviewed is included below:
2018 Report 1: Building health systems for better outcomes
Survey data
In the first report of the Future Health Index in 2018, we analyzed 45 different metrics and grouped them together in key pillars: 1. Value Measure The Value Measure is a new indicator of the value delivered by healthcare systems of developed and developing markets. It combines factors associated with value-based care and access to care, arguably the ultimate goals of modern healthcare. It consists of three parts: 1. Access (i.e. how universal, and affordable, is access to healthcare in the designated market?) 2. Satisfaction (i.e. to what extent do the general population and practitioners in the designated market see the healthcare system as trustworthy, and effective?) 3. Efficiency (i.e. does the system in the given market produce outcomes at an optimum cost?) The second pillar, Current State measures current levels of adoption of key digital enablers: 1. Data (collection and analytics) (including wearables, Electronic Health Records (EHRs), Intelligent Care) 2. Care Delivery (Telehealth and Diagnostic & Treatment Solutions) Each pillar consists of several sub-metrics. Within each pillar, the metrics are normalized to ensure comparability across countries and are scored to fit onto a 0 to 100 scale. Specifically, metrics related to market size are normalized per capita, per hospital bed or per physician in each country. The market size metrics were scored relative to the highest scoring country (with a population over 1,000,000) among the available dataset. For other metrics, including those for the Value Measure and technology infrastructure metrics, scoring is either relative to the highest scoring country (with a population over 1,000,000) among the available dataset, or, based on any optimal baseline number set by global authorities e.g. standards/goals set by the United Nations Sustainable Development Goals (SDGs). By excluding countries with less than 1,000,000 population, we exclude outliers which may create unrealistic potential to reach 100. A metric which does not follow this pattern of normalization is: In a next step, the scores for each metric are then averaged to calculate each sub-index score and those sub-indices averaged to create each pillar.
2. Current State (of Data and Care Delivery)
The risk of impoverishment due to surgical care – this metric is reported as a percentage, so it is simply inversed and no further normalization is needed.
The 45 individual metrics analyzed use a combination of third-party data and original research collected via a survey conducted in 2017 and 2018 in partnership with a global market research firm (see survey details below).
2017 Report: Care that delivers
Survey data
The survey data was collected January 18, 2017 to March 3, 2017 for 15 of the 16 countries analyzed in 2018 (Australia, Brazil, China, France, Germany, Italy, The Netherlands, Russia, Saudi Arabia, Singapore, South Africa, Spain, Sweden, U.K. and U.S.) in their native language. Survey data for India was collected during February 16 to March 26, 2018 in a manner consistent with the other countries in 2017. The survey had an average length of 25-30 minutes. A combination of online, face-to-face (computer-assisted) and phone (computer-assisted) interviewing was used.
The total sample from the survey includes:
The full 2017 methodology is available in the 2017 report.
2016 Report: The capacity to care
Survey data
The survey data was collected February 24, 2016 to April 8, 2016 in 13 countries (Australia, Brazil, China, France, Germany, Japan, The Netherlands, Singapore, South Africa, Sweden, UAE, U.K. and U.S.) in their native language. The survey had an average length of 25-30 minutes. A combination of online, face-to-face (computer-assisted) and phone (computer-assisted) interviewing was used.
The full 2016 methodology is available in the 2016 report.